It’s hard to believe that half of the project is already over!! Apologies for the lack of posts – It’s been hard to document exactly what I’ve been doing because much of my role hasn’t been tangible.
To summarize, I came to India at the beginning of October with rough ideas of how our team of 16 volunteers could contribute to Samuha Samarthya in a sustainable way. Don’t get me wrong – Samarthya is doing an INCREDIBLE job, helping hundreds of children through their various programs. They are one of the most dedicated organizations in the state of Karnataka (and won an award last year for it!).
As an international volunteer, it was so tempting to fly in, help a bunch of patients, get that happy feeling inside because you’re helping these super-cute amazing kids and lovely adults, and then fly out, but that would have left the organization no better than when we found it.
Here were our original goals:
- Improve the Community-Based Rehabilitation (CBR) training manuals (which haven’t been updated in 20 years!)
- Hold theoretical and practical educational sessions for the CBR workers to improve and standardize the level of care being provided in the Early Intervention Centres, the Spinal Cord Rehabilitation Unit, and other community outreach programs.
- Hold educational sessions for caregivers, school teachers, and other community members to maximize care and inclusion of people with disabilities in these rural communities.
- Increase efficiency of the organization by piloting and implementing new ventures such as a loan equipment program
- Teach the local CBR-Workers to be teachers, so they can continue to educate their colleagues and future newcomers to the field, and not rely on Canadian volunteers for education
- Raise awareness of Samuha Samarthya by facilitating Canadian volunteer experiences (physiotherapists and orthotists). There are a total of 17 other clinicians and students coming for 1-2 month stints throughout the project!
- Raise awareness for global health and create avenues for discussion about international volunteering in general, as I hope some of these volunteers may have the desire to contribute to other international projects. It is crucial to understand what type of volunteer work is beneficial for these types of NGOs, as we will be aiming to empower the local workers rather than doing the clinical work ourselves. We don’t want to parachute in, work, and leave, as that would leave the organization no different than when we found it.
Things changed from the second we hit the ground. It quickly became much more complicated as I peeled back the onion and found layers and layers of issues… and it took the whole first two months to really suss out what was happening at Samarthya. During that time, I really got to know the staff at a personal level and they shared their joys and challenges of their jobs. Through these conversations, I was able to gain their trust so they might be more open to our suggestions over the six month period.
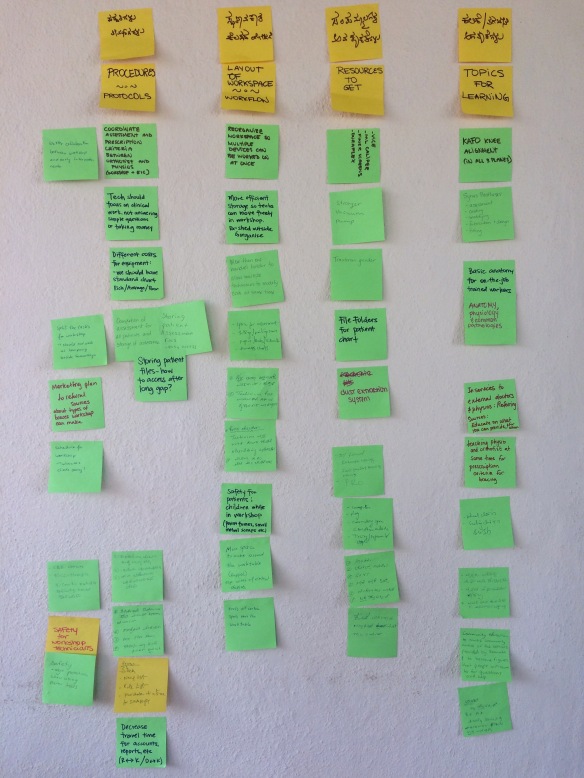
Phase 1 (Oct-Nov): The first group of volunteers (Jen Tam and Julie Alexander) played vital roles in observing and inquiring about the technical skills, procedures, systems, and team dynamics. They asked why, why, why for each issue that came up, and found multiple levels which needed some work.
Here was the tricky part that applied to all goals: what level could we realistically affect in the 6 months to create a lasting change? Some issues were quick fixes (ie, implementing referral sheets to send clients to the workshop for splints) and some issues were stemmed as high as the board level. We couldn’t tackle it all.
Let’s look at goals number 1 & 2 for now – in October we started looking at the old training manuals and agreed that they needed to be updated. In addition, several junior workers had been hired recently and they hadn’t been trained formally yet in theory or practical skills. So as we were researching the information to update in the manuals, we were spending time observing and working with the CBR workers.
Challenge #1 – There wasn’t a standardized level of knowledge among the staff, so what was the appropriate level of difficulty to include in these manuals?
Challenge #2 – All CBR-workers were full to the brim with work and they wouldn’t have time to study these manuals. Why were they so busy?
Challenge #3 – Inefficiency. High-skilled people were doing low-skilled jobs; there was no designated administration person so the senior therapists were doing things like computer data entry, scheduling clients, and settling bills, and therefore clients couldn’t be seen. Additionally, it seemed like other processes were taking 2-3 steps more than required.
Because of this, seniors didn’t have time to train the juniors, and therefore the juniors weren’t capable to help with the high volume of clients.
NEW GOAL: Create a 6-month training schedules for the Early Intervention Center with set teaching modules for senior therapists to train the junior therapists in-house, so seniors could be free to do other much-needed work. Our goal is to streamline some Early Intervention processes = more free time for seniors = more opportunity to train juniors = spread out the workload and ensure a succession plan for the future.
Additionally, there were no therapists that were formally trained for the Spinal Cord Rehab unit. ADDED GOAL: Create a training manual and provide educational sessions about spinal cord injury to educate two new therapists who will run camps for men with spinal cord injuries.
Phase 2 (Dec): Physio Jen Waring observed and surveyed the junior workers, asked them what areas they wanted more knowledge in, updated a skeleton of the training manual and suggested a 6-month training plan. Physios Sarah Monsees and Larissa Vassos were based in the Spinal Cord Rehab Center and created a 30-page manual, starting with basic theory of spine anatomy, nervous systems, and more. They ran multiple evening teaching sessions a week that dramatically increased local workers Channappa and Meheboob’s knowledge and skills, and helped them run a 1-month camp for four men with spinal cord injuries. They also created exercise boards to help with compliance in the gym. 


The volunteers have exercised skills FAR beyond physiotherapy. We’ve been challenged with curriculum development, teaching, organizational development, people management, budgeting, and of course, doing all of the above across a language barrier.
Thanks Jen, Sarah, and Larissa for ensuring success in Phase 2!!
Next update: Scrapping goal #4, delaying goals #3 & 5, and adding very important goal #8!















 Prabhakar’s dream is to have multiple clinic spaces (currently only one treatment room) staffed by three assistants, and to hire a recruiter to visit villages, meet with doctors and other health care professionals, and provide simple education sessions to surrounding community members.
Prabhakar’s dream is to have multiple clinic spaces (currently only one treatment room) staffed by three assistants, and to hire a recruiter to visit villages, meet with doctors and other health care professionals, and provide simple education sessions to surrounding community members.













{kind=link}